The ICELL8 Single-Cell System is an open platform scientists are using to develop customized protocols, and we are very excited about the collaborations forming as a result of the system's flexibility. Takara Bio R&D scientists Kazu Tori and Montse Morell visited the Max Planck Institute for Heart and Lung Research in Bad Nauheim, Germany, to be trained by Dr. Stefan Günther of the Thomas Braun lab on a protocol they developed (Yekelchyk et al. 2019) for the preparation of cardiomyocytes for processing on the ICELL8 Single-Cell System. We are thankful for the team's hard work and willingness to share their workflow with us and other ICELL8 system users.
Primary adult mouse cardiomyocytes are a challenging cell type to capture, as they are delicate, sometimes multinucleated, and difficult to isolate as a pure population. They are also very large, and therefore a good candidate for isolation with the ICELL8 system dispenser's wide-bore nozzles. Furthermore, the ICELL8 system allows the user to visualize an isolated cardiomyocyte in a well and decide whether to process it. This protocol describes the isolation of cardiomyocytes from an adult mouse heart in preparation for dispensing and analysis on the ICELL8 system. The isolation protocol is mainly adapted from the published work by O'Connell, Rodrigo, and Simpson in 2007. If you wish to implement this protocol on the ICELL8 cx Single-Cell System, please contact your FSE.
Protocol
A. Prior to isolation
The formulation of the Perfusion Buffer in this protocol differs slightly from the O'Connell protocol. (Please see the recipe, below.) The total volume of Perfusion Buffer to be prepared will be twice the capacity (in ml) of your chosen perfusion apparatus plus 10 ml. The following buffer is used during the whole process, but with different additives at various points.
NOTE: BDM is used to decrease the contraction of the heart. The absence of Ca2+ is also important throughout the whole isolation process.
B. Collecting the sample
To aid the user in performing this subprotocol, here is a similar visual protocol (Judd, Lovas, and Huang 2016). Before beginning this subprotocol, prepare enough Perfusion Buffer for your perfusion apparatus. Also, prepare an equivalent volume of Digestion Buffer (for tissue digestion) by resuspending Liberase enzyme in Perfusion Buffer to a final concentration of 0.25 mg/ml and place on ice. Additionally, prepare 10 ml of Perfusion Buffer with 10% calf serum (for stopping digestion) and place on ice.
Perform a peritoneal injection of heparin and anesthesia to the mouse. After the mouse is unconscious, extract the heart, ligate the right ventricle, and introduce a cannula in the aorta (so that the tip of the cannula is just above the aortic valve). Immediately start the perfusion with the Perfusion Buffer.
Approximately 30 min after the start of perfusion, when the perfusion flow is faster, begin the digestion by exchanging the Digestion Buffer with the running Perfusion Buffer.
Check the progress of digestion by looking at the flowthrough under the microscope for the presence of dissociated cells. The total digestion time will depend on the heart properties (mouse age, fibrotic stage, etc.) When rod-shaped single cells are present, and the heart looks pale, swollen, and flaccid, please proceed to the next step.
At this point, remove the heart from the perfusion apparatus and place it in a watch glass containing 10 ml of Digestion Buffer.
Carefully dissolve the heart by teasing it apart with tweezers and pipetting the buffer onto the tissue very slowly and gently with a 10-ml pipette. Cardiomyocytes are extremely delicate, so avoid vigorous pipetting.
Transfer the solution to a 50-ml Falcon tube. Add the same volume of fresh Perfusion Buffer + serum (prepared earlier) to stop the digestion. The final concentration of serum should be 5%.
After a few minutes, the majority of the cardiomyocytes will settle to the bottom. Carefully transfer the majority of the supernatant (containing additional cardiomyocytes) to a 15-ml tube and centrifuge at 500g for 1 min. This step is performed so as to recover as many cardiomyocytes as possible.
Decant off the supernatant (contains smooth muscle cells and fibroblasts) and pour the obtained pellet into the 50-ml tube from Step 6.
Count the cells using a Sedgewick-Rafter counting chamberor a standard hemocytometer using a 1:100 dilution of the cell suspension in buffer. Under the microscope, rod-shaped and round cells will be detected along with some cell debris. Only the rod-shaped cells should be considered healthy cardiomyocytes and, in a good sample, the percentage of rod-shaped cells should be higher than round cells. Write down the cell count here, as it may be useful later in Step C.5.a.
C. Staining and counting cells
Perform the cell staining for a total of 5 min at room temperature. Add 1 µM CellTracker dye (1:1,000 of 1-mM stock) to label the cellular cytoplasm and Hoechst dye (1 drop per ml) to the cell suspension. If the cells start to sediment, invert the tube after dye addition; do not pipette.
Wash the cells with Perfusion Buffer. Centrifuge the cells at 100g for 30 sec, and then pipette off the supernatant. (Alternatively, let the cardiomyocytes settle down for approximately 5 min at room temperature.) Add 1 ml of Perfusion Buffer then invert to resuspend (do not pipette). Repeat the wash twice with 1 ml of Perfusion Buffer for each wash.
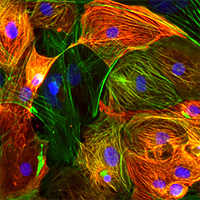
OPTIONAL: Check the staining under a fluorescence microscope, if desired. The cell cytoplasms should be red, and the nuclei should be blue.
A final cell concentration is needed to calculate the dilution of cells for dispensing. Note the total volume of the cell suspension. Count the cells using one of the following options:
Theoretical calculation: the survival rate throughout the isolation process tends to be about 40%, so the final cell number for dispensing can be calculated based on the following formula, which uses the initial cell count obtained after isolation in Step B.10.
final cell concentration = (c * 0.375) (u / f)
c = initial number of cells/ml, counted in Step B.10 f = ml, final volume for resuspension of cells after washing u = ml, volume used for staining (e.g., 2 ml)
Actual count: counting chamber or standard hemocytometer.
D. Dispensing cells
Please refer to operation and dispensing instructions in the ICELL8 system user manual.
Dilute the cells before dispensing to achieve a lambda of 0.25 (in other words, 1 cell per 200 nl). To prepare 1 ml of this solution, use 0.4 U/µl RNase Inhibitor and 5X Second Diluent.
NOTES:
The lambda used for cardiomyocytes is lower than usual for other cell types. Also, the concentration of diluent is higher than usual.
For negative and positive controls, use 0.4 U/µl RNase Inhibitor and 1X Second Diluent as in the user manual.
Prepare the source plate by adding 35 μl of cell suspension to each of the 8 sample wells. Add fiducial mix and negative and positive controls to the source plate.
Add a pause step during the sample dispensing process by selecting the proper option in the software. After the first dispense, the software will display a message alerting the user that the pause has been activated. At this time, remove the source plate from the dispensing platform and replace the cell suspension with 35 µl of fresh cell suspension in each of the 8 sample wells, and carefully put the source plate back onto the dispensing platform.
NOTE: Pausing may work differently for the ICELL8 cx Single-Cell System. Please contact your FSE for support.
Next, press [Start] to resume the protocol. The pause prompt will reappear one more time; after the pause, discard the cell suspension in all wells and add another 35 µl/well of fresh cell suspension. Try to minimize the wait time between pipetting and dispensing of cells.
IMPORTANT: This step is essential. Due to the size of cardiomyocytes, cells will quickly settle to the bottom; if the pause steps are not introduced, many cells will be aspirated in the first dispense, causing an unequal distribution (Figure 1).
Figure 1. The image above depicts in gray the distribution of wells containing cells with and without the pause steps. Adding the pause steps results in significantly better cell capture.
When all dispenses are complete, spin the plate at 300g for 3 min and proceed with imaging.
E. Imaging and manual triage
Refer to the manual triage instructions in the imaging software user manual.
Adjust the channel settings for detection of CellTracker dye: set "gamma" to 0.8 and the "MinAutoContrastRange" to 255. The preset "DAPI" and "Texas Red" channels will not be used for this protocol. The exposure in the red channel can be adjusted for optimal visualization.
Figure 2. Visualization of a rod-shaped, multinucleated cardiomyocyte in one well.
NOTE: A typical ratio of binucleated to mononucleated cardiomyocytes is 80/20. The following criteria are suggested for manual triage: mono-, bi-, or multi-nucleated cells should have a rod shape; nuclei must overlap with the cytoplasm.
F. Preparing the library
Please refer to the ICELL8 3' DE Kit User Manual for detailed library prep instructions. For this protocol, use the following modifications:
During cell lysis, perform a preheat step by heating the chip at 72°C for 5 min, and then immediately place it on ice. This is important for optimal cell lysis.
Prepare the RT-PCR reaction with 2X concentration of Triton X-100.
Materials required
Perfusion buffer ingredients, including 2,3-Butanedione monoxime (Sigma-Aldrich, Cat. # B0753)
Liberase T-Flex, Research Grade (Roche, Cat. # 05989132001)
CellTracker Red CMTPX Dye (Thermo Fisher Scientific, Cat. # C34552)
References
Judd, J., Lovas, J. & Huang, G. N. Isolation, Culture and Transduction of Adult Mouse Cardiomyocytes. J. Vis. Exp. (2016). Watch the visual protocol »
O'Connell, T. D., Rodrigo, M. C. & Simpson, P. C. in Cardiovasc.Proteomics 271–296 (Humana Press, 2007).
Yekelchyk, M., Guenther, S., Preussner, J. & Braun, T. Mono- and multi-nucleated ventricular cardiomyocytes constitute a transcriptionally homogenous cell population. Basic Res. Cardiol.114, 36 (2019). Read the paper »
User-generated protocols
User-generated protocols are based on internal proof-of-concept experiments, customer collaborations, and published literature. In some cases, relevant results are discussed in our research news BioView blog articles. While we expect these protocols to be successful in your hands, they may not be fully reviewed or optimized. We encourage you to contact us or refer to the published literature for more information about these user-generated and -reported protocols.
If you are looking for a product-specific, fully optimized User Manual or Protocol-At-A-Glance, please visit the product's product page, open the item's product details row in the price table, and click Documents. More detailed instructions for locating documents are available on our website FAQs page.
Questions? Protocols of your own that you would like to share?